


















Promotion of this article has been funded by AstraZeneca UK, who had no influence on the authors or content, and reviewed for accuracy purposes only. This article is for HCPs and subscribers of HSJ only.
Sponsored by and written for
The current national situation
Through the 10-Year Health Plan:Fit for the Future, the UK government and the NHS have committed to redesigning patient care pathways to reduce hospital admissions and embed a focus on risk-based care.1,2
Within these long-term ambitions, respiratory disease has been identified as a key clinical priority.3 In England, more than 1.2 million people are living with a diagnosis of chronic obstructive pulmonary disease (COPD).4 Many of these patients live with multiple comorbidities, which increase clinical complexity and heighten the risks associated with COPD, making disease management more challenging.5
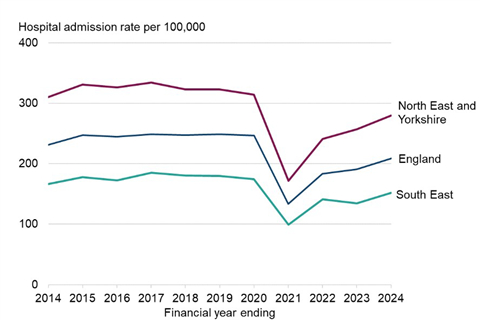
The burden of COPD on the NHS is considerable. Between 2023 and 2024, there were 121,129 COPD-related emergency hospitalisation admissions in England (Figure 1), representing a 9 per cent increase compared with the previous year.6 This has placed additional pressure on already strained emergency departments (EDs). More broadly, the NHS has been unable to consistently meet the four-hour standard for admission, referral or discharge since 2015, reflecting systemic pressures including overwhelmed ED services and suboptimal hospital flow.7
Improving COPD management, therefore, is an important opportunity to support delivery of the NHS’s strategic priorities. Several initiatives are already underway, such as the launch of the Respiratory Transformation Partnership announced in March 2026,9 (which includes AstraZeneca as a partner) featuring dedicated COPD workstreams; the inclusion of COPD within the 2026/27 Neighbourhood Health Framework;10 the introduction of best practice tariffs for COPD discharge care;11 and new COPD commissioning guidance that emphasises proactive care and risk stratification within service design.12
The situation at Royal Stoke University Hospital
This national focus on improving respiratory care is already being translated into practice at a local level. At Royal Stoke University Hospital, part of Staffordshire and Stoke-on-Trent Integrated Care Board, where COPD prevalence is among the highest in England, targeted efforts have been made to address longstanding challenges in patient management.5
Historically, the large volume of patients with COPD meant individuals admitted to the hospital were often lost within the system, contributing to delayed transfers of care. High staff turnover further compounded these issues by limiting access to specialist respiratory nurses. In the absence of a clear pathway, many patients were assessed and discharged without appropriate specialist input. In response, a project was initiated to embed specialist care at the front end of a structured COPD pathway supported by AstraZeneca via a donated service.
The solution: High Risk of Delayed Transfer (HRD) flow tool
Central to this approach is the HRD flow tool. This tool identifies patients at the point of admission to the ED by linking ED disease codes with primary care data, specifically COPD Quality and Outcomes Framework (QOF) coding. Once identified, patients undergo digital triage by a specialist nurse, followed by clinical review.
By enabling real-time identification and tracking of patients with COPD exacerbations across the hospital, the HRD flow tool supports efficient use of clinical resources. It eliminates the need for manual ward searches, facilitates proactive specialist review, and enables earlier discharge planning, helping to alleviate pressure on the ED.
The pathway also extends beyond initial presentation. Patients who attend the ED with breathing difficulties out of hours or miss specialist input are automatically flagged by the HRD flow tool and invited to a “hot clinic” within 14 days. At this clinic, patients without a prior diagnosis of COPD and who have a history of smoking in their primary care record undergo spirometry and clinical assessment to confirm or exclude COPD, while those with an existing diagnosis of COPD receive treatment optimisation aimed at reducing future exacerbations and hospital attendance. Patients who smoke and present with exacerbations are also proactively followed up, ensuring a more comprehensive and preventative approach to care.
The impact of the HRD flow tool
Despite a 20 per cent reduction in the number of specialist nurses at Royal Stoke, the HRD flow tool has allowed the team to maintain patient review numbers and performance levels by saving an average of two to three hours per day. The increase in specialist nurse capacity has meant patients with COPD can now be diverted away from the ED, freeing up time for a new outpatient follow‑up clinic for patients with COPD exacerbations.
The HRD flow tool has also impacted primary care, where “hot clinics” have been running for more than four months. The local GP federation provided administrative support to organise the community clinic, where patient reviews are recorded directly in electronic patient records using a read‑coded, QOF‑aligned template. This removes the need for annual review and has so far saved over 40.5 hours of primary care clinical time thus creating a winning formula for all patients and organisations involved.
In addition, local community trusts are reviewing patients unable to travel, and local GP teams have agreed to follow up on sputum and blood test results and allow prescribing through their own clinical systems. Further extensive collaboration with information governance teams has enabled primary, community and secondary care services to work together more effectively, improving integration across patient care pathways.
The future
If the local systems are to deliver on national priorities for prevention, urgent care reform and reduced hospital utilisation, they must redesign activity around the specialist workforce required to sustain integrated COPD care. At Royal Stoke University Hospital, embedding specialist respiratory services through the HRD flow tool has improved patient identification, enabled earlier discharge planning and saved nurses two to three hours per day, while supporting “hot clinic” follow-up services.
Building on this progress will require targeted investment to expand specialist nursing and respiratory service capacity, alongside a review of roles across hospital and community care to sustain and extend this approach. Scaling similar data-driven, specialist-led pathways across high-burden areas would support the delivery of national ambitions while improving care for patients with respiratory disease.
Veeva ID: GB-78116
Date of preparation: July 2026
Acknowledgements
The HRD-flow tool has been developed in-house by the Trust’s business intelligence team. Thomas Hill is the data architect for this project and has been critical to its development and success.
The wider team, including Keele University, led by Kelvin Jordan, local councils, commissioning support unit, transformation delivery unit, project management office, ICB, information services, information governance teams, and Graphnet, are also noted for their contributions. This work could not have happened without continued sponsorship and support from University Hospitals of North Midlands charity, the North Staffs Medical Institute and ARC (Applied Research Collaborations-NIHR) funding.
The authors would like to acknowledge the contributions of Ian Gibson, Tracey Lawton and the wider team at North Staffs GP Federation; Vicki Capewell, Georgie Woodcock and the wider team at Midlands Partnership University Foundation Trust; Jaqui Wade, Zarah Kahn and Ethan Harvey from the TDU; and Caroline Meredith, Vicki Poole, Ian Cliff and Michael Hepple, together with their respective teams, for their support in the implementation of the pathway.
The authors also acknowledge Karen Jackson, COPD clinical nurse specialist at Royal Stoke University Hospital, whose expertise and insights supported the development of this article and implementation of the pathway; Louise Goswell, pathway manager at AstraZeneca, for facilitating the creation of this article and supporting pathway implementation; and Fraser Collins and Jane Juif, Lucid Group Communications Ltd, for editorial support.
References
1. NHS England. Medium Term Planning Framework – delivering change together 2026/27 to 2028/29. www.england.nhs.uk/long-read/medium-term-planning-framework-delivering-change-together-2026-27-to-2028-29/. 28 October 2025. Accessed May 2026.
2. NHS England. 1 April 2026 next steps on planning and priorities for 2026/27. www.england.nhs.uk/long-read/1-april-2026-next-steps-on-planning-and-priorities-for-2026-27/. 17 April 2026. Accessed May 2026.
3. NHS England. Respiratory disease. https://www.england.nhs.uk/ourwork/clinical-policy/respiratory-disease/. Accessed May 2026.
4. Department of Health & Social Care. Public health profiles. https://fingertips.phe.org.uk/search/chronic%20obstructive%20pulmonary%20disease#page/4/gid/1/pat/159/par/K02000001/ati/15/are/E92000001/iid/253/age/1/sex/4/cat/-1/ctp/-1/yrr/1/cid/4/tbm/1. Accessed May 2026.
5. Staffordshire and Stoke-on-Trent ICB. All age respiratory strategy, 2025–30. https://staffsstoke.icb.nhs.uk/your-nhs-integrated-care-board/our-publications/plans-and-strategies/all-age-respiratory-strategy-final/?layout=file#:~:text=11-,Prevention,are%20both%20important%20to%20improve. 24 April 2025. Accessed May 2026.
6. Office for Health Improvement & Disparities. Respiratory disease profile: statistical commentary, June 2025. https://www.gov.uk/government/statistics/update-of-indicators-in-the-respiratory-disease-profile-june-2025/respiratory-disease-profile-statistical-commentary-june-2025. 3 June 2025. Accessed May 2026.
7. UK Government and NHS. NHS 10 Year Health Plan: Fit for the Future. https://assets.publishing.service.gov.uk/media/6888a0b1a11f859994409147/fit-for-the-future-10-year-health-plan-for-england.pdf. July 2025. Accessed May 2026.
8. Open Government Licence for public sector information. https://www.nationalarchives.gov.uk/doc/open-government-licence/version/3/. Accessed May 2026.
9. GOV.UK. Asthma and COPD patients to receive better care closer to home. www.gov.uk/government/news/asthma-and-copd-patients-to-receive-better-care-closer-to-home. 17 March 2026. Accessed May 2026.
10. GOV.UK. Neighbourhood health framework. www.gov.uk/government/publications/neighbourhood-health-framework. 17 March 2026. Accessed May 2026.
11. NHS England. Annex C: Guidance on best practice tariffs. www.england.nhs.uk/wp-content/uploads/2026/03/26-27NHSPS-Annex-C-Best-practice-tariffs.pdf. 2026. Accessed May 2026.
12. NHS England. Chronic obstructive pulmonary disease: commissioning strategies and resources. https://www.england.nhs.uk/long-read/copd-commissioning-strategies-resources/. Accessed May 2026.




