

















Partnership working has been vital to delivering a co-ordinated 24-hour palliative care service, write Annie Macleod and Nicky Bannister.
Bedfordshire has established a single telephone number for all palliative care using a shared electronic record. This centre is open 24/7 year round and is at the heart the Partnerships for Excellence in Palliative Support service, which co-ordinates palliative care for patients, families, carers and health and social care staff.
Led by NHS Bedfordshire and Sue Ryder, 15 organisations are working in partnership to improve the experience and continuity of care for patients in their last 12 months of life. PEPS also supports generalist health and social care professionals to provide care at the patients’ place of choice – usually their home.
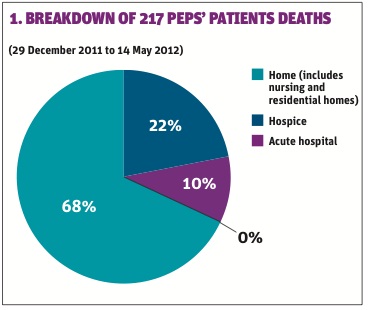
In the first five months of operation, PEPS has co-ordinated the care of 415 patients, 68 per cent of whom died at home, as they wanted. Only 10 per cent died in hospital.
Bedfordshire PEPS comprises the following organisations
- Sue Ryder-St John’s Hospice
- NHS Bedfordshire
- South Essex Partnership University Foundation Trust
- Keech Hospice Care
- Willen Hospice
- Garden House Hospice
- Florence Nightingale Hospice
- Bedford Day Care Hospice
- Bedford Borough Council
- Central Bedfordshire Council
- East of England Ambulance Trust
- Cambridgeshire Community Services
- Bedford Hospital Trust
- Luton and Dunstable Hospital Foundation Trust
- Marie Curie
The PEPS co-ordination centre manages the electronic palliative care co-ordination system and, with the patients’ consent, enables sharing of information.
Senior nurses are the first point of contact on the phone, so the most appropriate health or social care professional is identified to help patients in a timely manner.
Previously, services involved in caring for people at the end of life tended to work in isolation. There were several provider numbers to call, all of which had different operating times. That was confusing for patients, particularly out of hours. There was no central register for palliative care in the county.
Now, all organisations involved in providing palliative care across Bedfordshire have a single point of contact and an integrated co-ordinated service and information source. It aims to:
- Empower patients to be cared for in their preferred place.
- Provide high-quality care delivered by the right provider, in the right place, at the right time.
- Provide support and advice to the patients’ families and carers.
- Deliver improved outcomes and experience.
- Deliver the national quality target, SQU02, to increase deaths in usual home.
- Deliver the regional target to increase the number of patients held on the central end-of-life care register.
- Reduce expenditure on unplanned admissions, length of acute hospital stay and accident and emergency attendances.
The service is part of the quality, innovation, productivity and prevention programme for NHS Bedfordshire and plans to provide data to support palliative care service planning by future clinical commissioning groups. The initiative was proposed by the Palliative and End of Life Care Local Implementation Group, whose members are key partners and stakeholder organisations, including carer representatives who were instrumental in shaping the service.
While it is not legally binding, all organisations were asked to sign a memorandum of understanding as part of their commitment to PEPS. Individual meetings were set up with chief executives of each organisation to guide them through the model pathway and explain the role and commitment required.
A project group involving clinicians and operational representatives from the partner organisations was convened to develop an operational policy. This involved designing the route to access the service, the process of obtaining consent, information governance, establishing a data set for the PEPS information system and promoting the service. The group meets each month to review progress and highlight issues, so that operational policy can be revised as appropriate.
Overcoming challenges
Investing time in developing and building new working relationships between the organisations has been, and continues to be, vital to overcoming the challenges that have arisen, specifically:
- Developing an effective electronic system. SystmOne was felt to be the best option to host the register as the community teams were currently using it. However, it has required considerable work to reconfigure it to meet our needs. Those that don’t have access are exploring reader views. The local hospital is now exploring a read only SystmOne licence, which will allow clinicians using the PIMS system to search for patients registered with PEPS.
- We underestimated the work needed to raise awareness of PEPS and it will clearly need to continue. We have developed different resources to aid marketing. For example, a PEPS screensaver is circulating within the local hospital and PEPS staff are accessing local meetings and forums to promote the service.
Service evaluation
From 29 December 2011 to 14 May 2012, 415 patients have been registered on the information system for PEPS, 225 of whom are currently “active”. The support worker team has carried out 158 face-to-face visits. Capturing preferred and actual place of care and death is a service outcome that will be continually measured.
Figure 1 shows that 68 per cent of the 217 deceased patients were supported to die at home (this includes care homes). This closely mirrors 74 per cent of deceased patients stating their preferred place of death is “home”.
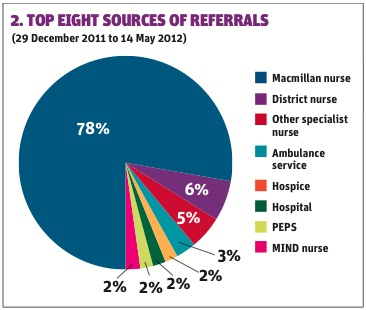
Figure 2 illustrates the top eight sources of referrals from professionals which result on data being included on the information system for PEPS, and is representative of the strong links established with the Macmillan team (78 per cent). Referrals from other sources, particularly district nurses, are increasing monthly as more work is done to raise awareness of the co-ordination centre.
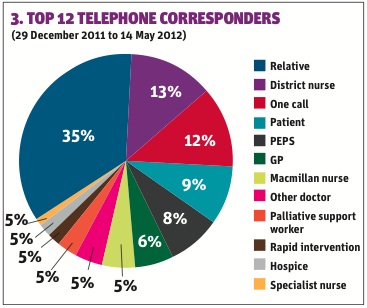
Figure 3 shows telephone activity illustrating the top 12 telephone corresponders. Aimed at supporting patients and families with a single number to contact, it is not surprising that the largest percentage (35 per cent) refers to patients’ relatives.
Other findings to date include:
- Hospital engagement has led to improved integration of acute and community care.
- The MDT team, through working with PEPS, are discharging patients home more rapidly.
- The co-ordination centre has been instrumental in supporting families between discharge and start of care package arrangements. Patients and families report feeling “secure” and “not feeling left alone”
- Feedback about the service has been “fantastic” from patients, their relatives and GPs.
The project is a 12-month pilot and we are evaluating the experience of our partner organisations. In addition, we are working with the School of Health and Related Research at Sheffield University to assess the economic impact of the service. The results will be available this month.
Find out more
Email annie.macleod@sueryder.org or nicky.bannister@bedfordshire.nhs.uk
getting to grips with the unplanned
Visit hsj.co.uk/southend
to find out how
an integrated approach has helped Southend Estuary CCG deal
with the challenging unplanned care agenda.
For more information email nicky.bannister@bedfordshire.nhs.uk or annie.macleod@sueryder.org.






{kind=link}
{kind=link}
{kind=link}
No comments yet