

















The unpredictable nature of trauma injuries has led one trust to call for an innovative approach to managing their surgical treatment. John Lloyd and colleagues explain how to cut overnight stays.
Accelerated recovery pathways and day surgery have revolutionised the management of a large proportion of elective orthopaedics. They allow a more efficient flow of patients through the system at lower cost in a reliable and predictable fashion. However, only sporadic examples exist for trauma.
Traditionally, trauma has not lent itself to a similar system because of its unpredictable nature. Patients present at unsociable times, often with concomitant injuries, and require differing levels of social support.
At Royal Bournemouth and Christchurch Hospitals and Poole Hospital foundation trusts have found greater patient satisfaction when patients wait at home rather than in hospital for their surgery. In 2008, our trauma department introduced a safe and reliable method of managing patients with ankle fractures at home while waiting for surgery. With ever increasing pressure on the trauma service and hospital beds, we decided to expand our day of surgery ankle fracture experience to other aspects of trauma.
The hospital trauma database was used to assess records on all trauma admissions over a seven month period prior to implementing the expanded trauma day of surgery scheme and then over the same seven month period two years later.
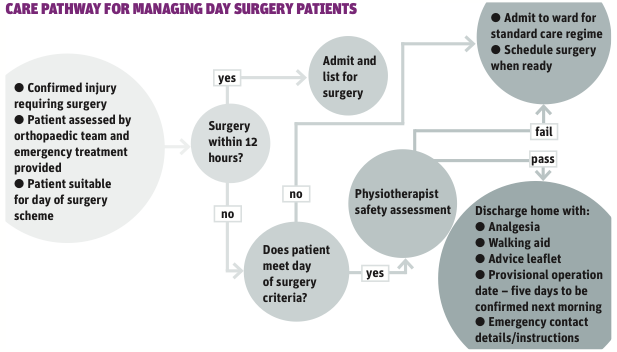
The flowchart (attached) shows the management pathway employed. Data was analysed on admission demographics, case mix, outliers, time from admission to surgery and length of stay. Inclusion criteria were:
- medically safe for discharge (ASA one and two);
- closed, neurovascularly intact injury that will not be adversely affected by waiting up to a maximum of 14 days;
- sufficiently comfortable with oral analgesia/plaster back slab;
- low risk of developing compartment syndrome;
- able to mobilise safely (non-weight bearing if appropriate);
- independent in activities of daily living;
- telephone at home;
- inside sanitation;
- within one hour of hospital;
- sufficient provisions of food and drink at home;
- compliant to follow instructions and advice;
- absence of previous thromboembolism.
Between April and October 2009, there were 1,703 trauma admissions, a mean of eight patients per day. Of these, 244 patients (14 per cent) were managed as day of surgery, 210 (12 per cent) were admitted from fracture clinic and 34 (2 per cent) were on the ankle home therapy scheme. None of the patients were discharged from the emergency department with a day of surgery admission plan.
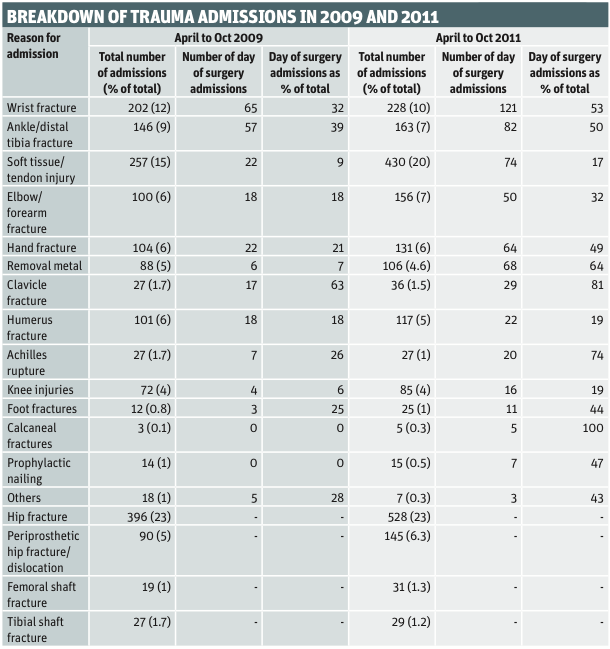
Two years later, between April and October 2011, there were 2,264 trauma admissions, a mean of 10.6 patients per day. Of these, 572 (25 per cent) patients were managed as day of surgery, 381 (17 per cent) were admitted from clinic, 18 (1 per cent) were on the ankle home therapy scheme and 173 (7 per cent) were discharged from the emergency department with a day of surgery plan. The table (right) shows the breakdown of trauma admissions by injury.
In 2009, 29 per cent of orthopaedic bed days relied on outlying orthopaedic patients. By 2011, this was only 9 per cent.
The mean time from admission to the operating theatre in 2009 was 38.6 hours for all trauma patients, and 14 hours for day of surgery patients, with 30 (12 per cent) waiting over 24 hours. There were 195 trauma patients, 11.5 per cent of the total, who were admitted, treated and discharged within 24 hours.
In 2011, the mean time from admission to the operating theatre was 25 hours for all trauma patients. The mean time to theatre for day of surgery patients was four hours, with 12 (2 per cent) waiting over 24 hours. There were 470 (20.8 per cent) trauma patients who were managed as day cases.
Positive impact
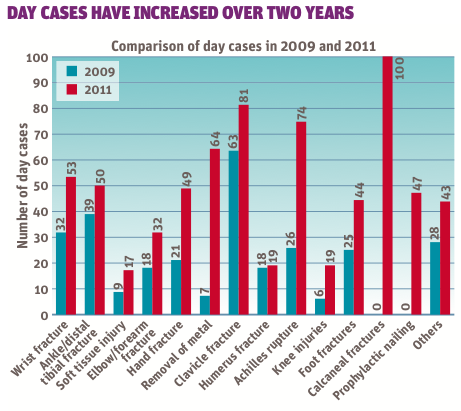
The results show that trauma admissions increased by 33 per cent over the two and a half years study period, but as the graph overleaf shows, the proportion of injuries has remained static.
During this same timeframe, the number of patients being managed on a day of surgery basis has risen to a quarter of all trauma admissions. Also the number of patients successfully treated as day cases – admitted, treated and discharged within 24 hours – has increased by 81 per cent over the study period.
These changes have had a positive impact on the number of orthopaedic outlying patients, which has seen a three-fold reduction. The efficiency of the system has also improved, with the mean time from admission to operation dropping from 14 hours for day of surgery patients to four hours, and the percentage of day of surgery patients failing to get to theatre within 24 hours falling six-fold to only 2 per cent.
A system like this can only run effectively with the correct infrastructure in place. Two essential components are clear management pathways and also the involvement of the trauma admission coordinator team. Laminated pathways are clearly available in the emergency department and trauma department. The three team members are experienced, qualified trauma nurses. They work a flexible working pattern so that at least one member is in the hospital from 7am-3.30pm Monday to Friday and also present for the weekend morning trauma meetings.
The trauma admission coordinator staff are an integral part of the service with no set ward commitment. They liaise with the day of surgery patients and coordinate and formulate the trauma lists in conjunction with the surgeon, anaesthetist, ward and theatre staff. They also compile the daily hospital trauma register and collect data for health initiatives, such as the national hip fracture registry.
Seasonal pressures
The home therapy management of patients awaiting ankle fracture fixation had proven to be successful, safe, cost effective and met with a high level of patient satisfaction.
Over time, there had been a slow expansion of this service for other trauma injury patients. However, it was not until December 2009, during an unexpectedly icy period, that the service was fully expanded. Over five days the trauma department experienced 20-30 admissions per day. This, combined with the usual seasonal bed pressures, put too great a strain on the existing service and emergency measures had to be taken. All patients who met the existing day case home management criteria were sent home from the emergency department after receiving initial assessment, diagnosis and emergency treatment. The duty orthopaedic doctor discussed their cases at the morning trauma meeting with the on-call consultant and a management plan was confirmed. The patient was contacted by one of the trauma admission coordinator team with plans for admission on the day of surgery or with a fracture clinic appointment.
A similar process occurs with the admission of patients from fracture clinic. In the past, patients were admitted from clinic to the ward where they would await surgery. Now, the team is contacted by the surgeon from clinic, with the patient details and management plan. If suitable, the patient goes home with a planned admission date to return on the day of surgery.
There were no reported adverse patient outcomes as a result of the day of surgery scheme. All patients received definitive surgery within the department’s pre-determined time of 14 days from the injury.
During the study period there has been no extra financial input in to the trauma service. The department staffing levels and levels of expertise have changed very little. Naturally, there will be the annual turnover of training grade medical, nursing and physiotherapy staff, but the numbers remained constant.
The overall numbers of operating lists have also remained constant. However, two of the original days involved three separate sessions. These have been amalgamated to allow two days with three sessions each. This has increased theatre efficiency and predictability when booking lists.
With such a complex, inter-related system such as trauma, it is difficult to attribute all improvements to the day of surgery system. It does, however, allow some control to be exerted over the unpredictable nature of trauma.
The ideal scenario would be to manage many more patients purely on a day case basis. It is still hugely under-utilised for trauma, despite the cost benefits. It is difficult to calculate savings, but we estimate at least annual savings of £141,428 from the increased use of day cases alone. This is based on patients not using a hospital bed overnight, which has a tariff cost of £300.
With the increase in number of day of surgery patients, we have found a greater number of trauma patients are admitted via the day surgery ward. Unfortunately, current resource allocation only allows the trauma service one specific day surgery list a week. This alternates between hand trauma and removal of metal work.
In the future, theatre use and allocation may be reassessed, but it does not currently stop some of our patients from being managed as day cases via the main trauma theatre lists. This requires greater planning by the trauma admission coordinator team. Problems with failure of discharge are often due to poor planning and lack of clear pathways rather than failure of the direct clinical care.
With the correct infrastructure in place, up to a quarter of trauma requiring surgery can avoid “routine” hospital admission and be managed at home until the day of surgery. This process also helps reduce orthopaedic outliers.
It is possible to organise day surgery lists, non-x-ray lists or surgeon case specific lists depending on the demand. Having a constant pool of patients waiting for surgery means that trauma lists can be optimised and managed in a very efficient and flexible manner.






{kind=link}
{kind=link}
{kind=link}
No comments yet