



















Why EPR programme design matters more than the technology itself
NHS organisations have made significant progress in deploying electronic patient records (EPRs). The question now is why many programmes have yet to fully realise the productivity, flow and experience improvements they promise.
Sponsored and written by
Analysis across international EPR programmes and broader enterprise transformations suggests that significant unrealised value remains within many NHS organisations. Benchmarking against BCG’s international database of transformation and EPR value realisation indicates that the average provider may still have up to £60m of operational and clinical value available through optimisation, workflow redesign and improved adoption.
Many NHS EPR programmes have understandably been structured around delivery plans, feature rollout and platform adoption, providing control during implementation. This can result in digitisation of current workflows, without realisation of additional value. There is a need to pivot focus so that progress is defined by clinical and operational impact, with programmes deliberately structured to translate functionality into measurable outcomes.
Delivery of value: EPR programmes have key characteristics of other complex enterprise transformations: multiyear, high-risk and requiring strong governance to succeed. However, once clinical care is added, the challenge becomes significantly more complex: outcomes are harder to define, variation in practice is greater, and the implications of design decisions directly impact patient care.
This is most visible in sequencing. Too often, deployment is driven by what can be built most easily rather than where value can be demonstrated early. A more effective approach starts by asking where deployment can build immediate clinical confidence and deliver tangible benefits.
High-acuity environments such as emergency care provide a natural starting point, forcing alignment with real workflows and exposing weaknesses quickly. When successful, they create trust that carries into subsequent phases. Modular delivery then allows organisations to absorb change incrementally, reducing risk and improving adoption. In this context, sequencing is not a technical decision, but a value one.
What it takes to succeed
Programmes that succeed take a different approach. Four characteristics consistently differentiate those that deliver value from those that do not:
1. Define outcomes first
They define a small number of outcomes and shape delivery around them. These are typically practical and measurable: time to complete tasks, pathway compliance and safety indicators. In this model, usability becomes a primary driver of value. If clinicians find a system slow or difficult to use, adoption drops and benefits fail to materialise. When workflows are intuitive and aligned to practice, administrative burden reduces, data quality improves, and patient flow becomes more predictable.
2. Embed measurement into governance
They embed measurement into governance rather than treating it as reporting. Metrics are aligned to outcomes, ensuring progress is defined by impact rather than completion. This changes behaviour. Decisions are prioritised based on expected value, reducing unnecessary configuration and limiting feature expansion. It also supports modular delivery, allowing organisations to build confidence as benefits are realised.
3. Standardise with purpose
They maintain disciplined standardisation. Excessive localisation increases technical debt, slows upgrades and fragments clinical practice. Leading international systems such as Kaiser Permanente, Intermountain and Santeon demonstrate that value is maximised where standardisation is combined with strong clinical ownership and transparent performance data. For NHS organisations, the opportunity is to apply these principles, not replicate the models directly.
4. Engage clinicians meaningfully
They invest in meaningful clinical engagement. Too often, clinicians are drawn into detailed design debates rather than shaping priorities. Effective engagement starts by identifying inefficiencies and linking them to measurable outcomes. Without this, organisations accumulate transformation debt. Automation and AI can reduce manual burden, but only when applied to well-designed processes.
Ultimately, these programmes are characterised by clear ownership. Leaders accountable for outcomes are embedded within governance, shaping decisions and managing trade-offs. Without this, accountability diffuses and progress slows.
Most clinical care is now delivered digitally, and productivity is the defining challenge facing the NHS. Digital represents one of the strongest opportunities to address it, but only if it is used differently. Looking ahead, EPRs will underpin more agentic models of care, where workflows are coordinated through automation, decision support and AI. The value of this shift will depend not on how much technology is deployed, but on how effectively it is embedded into clinical and operational practice.
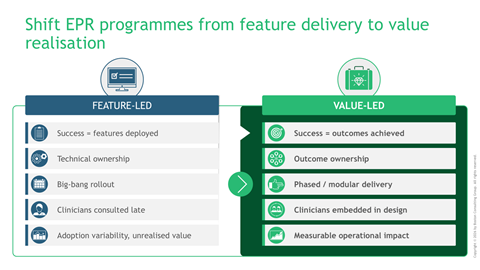
If success is measured by features delivered, value will fall short.
If success is measured by outcomes achieved, care will change.
EPRs are not the end of transformation but its foundation, requiring programmes structured differently, with clear ownership, deliberate sequencing and a focus on outcomes from the outset.
For a deeper look at this topic, please click here.








