


















Weak support services could be one of the greatest barriers to clinical commissioning groups’ success and undermine attempts to control spending, CCG leaders fear.

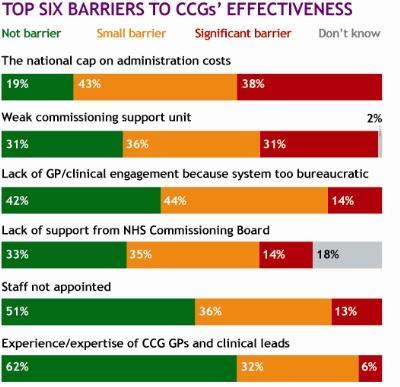
HSJ’s CCG Barometer survey asked leaders to rate potential barriers to their effectiveness as an organisation in the next year.
The most widely cited barriers were the national £25 per head limit on administration costs, followed by having a weak commissioning support unit, with 81 and 67 per cent or respondents respectively naming them as barriers. However, few CCGs appear poised to abandon their unit.
Asked whether their CCG might move a significant amount of commissioning support in-house in the next year, 20 per cent said it was likely and just 6 per cent very likely.
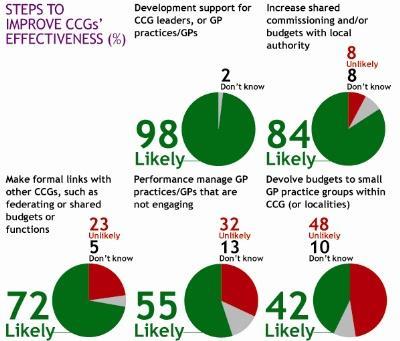
Nineteen per cent said they were likely to re-contract a significant amount of their support to alternative providers. Two per cent said they were very likely to do so.
NHS Kingston CCG accountable officer David Smith warned that many group leaders were concerned about their support units being under-developed as they begin contracting for 2013-14.
He said: “CSUs are really critical as they are going to be managing our acute budget. We are in the middle of the transition, and we are entering the next contracting round. A lot of people are concerned about that risk.”
Mr Smith said if support units did not prove themselves, CCGs would look for alternatives, but “if they can deliver I can’t see why they can’t be as effective as going to the market”.
Johnny Marshall, a GP and senior member of CCG representative body NHS Clinical Commissioners, said support units were a “pivotal part of the success of CCGs” and the survey showed they needed to “ensure they are raising their game” in providing what CCGs wanted.
Another factor leaders identified as a likely barrier to CCGs’ effectiveness was engagement of their member GP practices.
NHS Vale of York CCG accountable officer Mark Hayes said it was a challenge for many groups to “convince the bulk of GPs this is something they’ve got to get on board with, and which will benefit their patients”.
NHS Commissioning Board director of commissioning development Dame Barbara Hakin said the lack of confidence could be because CCGs were only now confirming the funding for NHS support units, so they have been slower to develop and employ staff.
Dame Barbara said: “CCGs recognise that support units are, like themselves, on a journey.” She said CCGs had been told to finalise funding by the end of this month, which would put the units “in a very strong position to move faster”.
Exclusive: CCG leaders favour integration over competition

The first survey of CCG leaders has found they want providers to work closer together
- 1
- 2
- Currently reading
CCG Barometer: 'Weak support' a major concern for clinical commissioners




5 Readers' comments