

















An ambitious study has set out to discover what makes high performing organisations fly above the rest. Naomi Chambers and colleagues reveal their findings.
Learning from successful healthcare organisations has never been more important. Building and sustaining high performance in healthcare is a tricky, messy, and complex business. There are the usual challenges of clinical quality, safety and the patient experience, maintaining internal business efficiency, building a culture of innovation, developing fruitful inter-organisation collaborations and responding to external economic and political pressures.
As Cardiff University professor of public sector management George Boyne has pointed out, organisations can also be visited by good luck or ill-fortune, or deemed to be straying from the “correct” managerial processes, as judged by powerful external stakeholders. Long term NHS watchers can no doubt call to mind organisations that are not necessarily either high performing or failing, but have had a spell of good or bad luck, and others that may score objectively well in some domains but are deemed maverick, awkward and not part of the Nicholson inner circle.
To avoid the subjectivity associated with selecting high profile favourites, or flash-in-the-pan brilliance, last year Manchester Business School took a balanced view across three perspectives, together with continuous high performance over time, in its identification of a cluster of 19 high performing NHS organisations. We wanted to see what – if anything – was different about them that others could learn from.
We have repeated this study, with a larger sample, to strengthen the impact of the findings. This time we identified 35 high performing organisations, and compared some of their characteristics with 33 others.
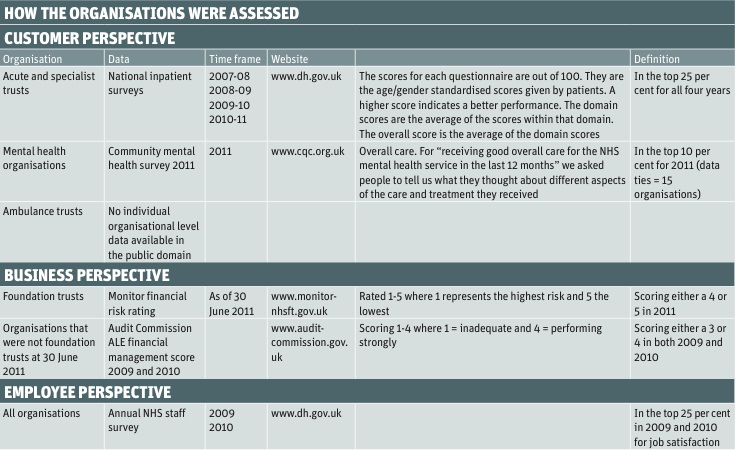
Because commissioning is in a state of flux, we included only provider organisations: specialist trusts, acute trusts and mental health trusts. We used the same three perspectives as last time: customer, business and employee.
We did consider adding an additional perspective on health outcomes. However, although there were a number of measures that we could have used for the specialist and acute trusts, it was not possible for us to find appropriate and comparable measures for mental health trusts. We would welcome advice on this for our study when repeated next year. This table identifies the process that we used.
Top performers, high performers and continuing high performers
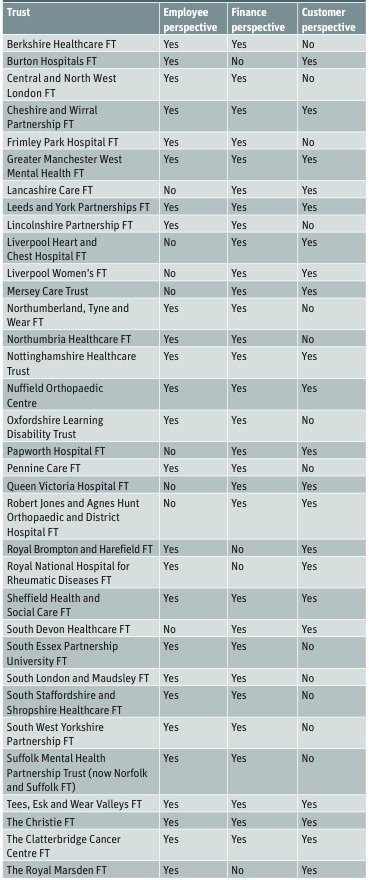
This year we can distinguish between nine top performing and a further 26 high performing organisations. The top performing organisations which scored highly across all three of the employee, customer and finance perspectives were:
- Cheshire and Wirral Partnership Foundation Trust;
- The Christie Foundation Trust;
- The Clatterbridge Cancer Centre Foundation Trust;
- Greater Manchester West Mental Health Foundation Trust;
- Leeds Partnerships Foundation Trust;
- Nottinghamshire Healthcare Trust;
- Nuffield Orthopaedic Centre Trust;
- Sheffield Health and Social Care Foundation Trust;
- Tees, Esk and Wear Valleys Foundation Trust.
A further 26 organisations were high performing across two of the three perspectives (see table, opposite page).
In general, specialist trusts and mental health trusts were over-represented in the high performance group; 55 per cent and 34 per cent, respectively, were categorised as high performing. Acute trusts were under-represented: none was in the “top performing” bracket, and just 2.7 per cent were categorised as “high performing”. If the types of trusts were evenly represented, there would be around 15.5 per cent of each type.
Our study last year came up with similar findings. The accusation can be levied that it is easier for smaller and more focused organisations to do better. If that is true, should we consider breaking up our monoliths, or at least subdividing them into separate operating units so that they can become these smaller, more focused and higher performing organisations?
Six of the 35 were also classified as high performing in last year’s study so we think these could be classified as continuing high performers:
- The Clatterbridge Cancer Centre Foundation Trust;
- The Christie Foundation Trust;
- Queen Victoria Hospital Foundation Trust;
- Royal Brompton and Harefield Foundation Trust;
- South Essex Partnership University Foundation Trust;
- The Royal Marsden Foundation Trust.
What did we find that distinguished these high performers from the others? We examined annual reports from the 2010-11 financial year and this time looked at three main factors: the gender balance on the board, financial turnover and staff sickness rates. In each case, the results are intriguing and surprising.
Key findings
The findings point to the following, which bear further debate and investigation:
- Although to be welcomed, a high proportion of women on boards may not be associated with superior organisation performance;
- Women chief executives may need additional support as they may, for whatever reason, be more likely to be at the helm of the more challenged trusts;
- Small, medium and super-sized NHS organisations may be equally viable;
- Getting to the heart of staff sickness absence would be a worthwhile endeavour in the interests of business efficiency, quality of care and organisation wellbeing.
Women on boards
Why investigate women on boards? There has been renewed interest recently in the business argument for increasing the proportion of women on boards. The Davies report in 2011 recommended that FTSE 100 companies have at least 25 per cent women on their boards by 2015. The “30 per cent club”, a group of chairs committed to bringing more women on to UK corporate boards, is voluntarily aiming for a higher proportion.
Our study last year noted that high performance might be associated with at least 50 per cent women on NHS boards. A US study of 1,500 companies published this year found that companies headed by a female chief executive had higher performance outcomes than others.
Our study this year found a surprisingly high proportion of women on boards. Women made up 39.7 per cent of board membership across all 68 organisations. There was a slightly lower proportion of women (37 per cent) on boards in the high performing as opposed to the not-so-high performing group (43 per cent) but this difference did not reach a statistical significance.
We also found that women were chief executives of 30 (44 per cent) of our 68 organisations. This compares very favourably with FTSE 100 companies which only have 14 per cent women as directors on their boards and only 10 per cent as chief executives. But women were only in charge of 12 (34 per cent) high performing organisations and were at the helm of 18 (55 per cent) of the others.
What does all this mean? The first observation is that the NHS can rightly be judged to be in the vanguard both in terms of board gender diversity and proportion of women as chief executives. But why are there more women running the not so successful NHS organisations? For example, is it easier for women to break the glass ceiling by going for the less attractive and more challenging posts? Do they focus on other means of added value or measures of performance to the detriment of national targets and measures, which means their organisations do not reach the high performing bar?
This warrants further investigation and we can only conjecture at this point.
Turnover
There has been much comment about the problems associated with mergers and acquisitions and diseconomies of scale. These currently revolve around the acquisition of community services by acute and mental health trusts as a result of the total separation of healthcare commissioning from provision in England. Mergers now involve the takeover of hospitals not considered viable in their own right as standalone foundation trusts.
We therefore wanted to find out whether size matters. Is there a gradual diseconomy of scale or indeed a “sweet spot”?
We plotted the size of organisations as measured by income and whether they were high performing. We could not find an association here – it appears that neither small nor big is necessarily beautiful. And although mergers and acquisitions may prove a harmful distraction in terms of potential disruptions to organisation memory, performance improvement and so on, size as expressed in financial turnover does not appear to be an issue. Equally, small organisations should not be regarded necessarily as non-viable (see graph, above).
Staff sickness
The third area we investigated was staff absence through sickness. We hypothesised that the high performing organisations would have a lower sickness absence rate. We would argue that staff absence rates, as well as an indicator of efficiency in human resources (the cost of absence per employee in the public sector is estimated by the Chartered Institute of Personnel and Development to be in the region of £800), can also be seen as a barometer of staff health and wellbeing and therefore of organisational wellbeing.
CIPD figures from their 2011 survey indicate that sickness rates may be approximately 3.1 per cent in the private sector, 4 per cent in the public sector, and 4.6 per cent in the health sector. Our findings were a surprise to us: in the high performing organisations, sickness absence rates varied from 2-7 per cent with an average of 4.3 per cent, and in the others sickness absence rates ranged from 3-6 per cent with an average of 4.2 per cent.
These rates are marginally lower than the CIPD findings, and, interestingly, there is no difference between the high performing organisations and the others. We can speculate as to the reason: in well managed organisations, do staff who do need to be off, because they are unwell, stay away appropriately supported by their organisation? And in more stretched organisations, do they come in to work when they are sick?
But, given that the most common cause of long term absence is stress and mental ill-health, do the findings alternatively suggest that the high performing organisations are as “stressed” as the others and that this high performance comes at a cost?
What do these findings add up to? We do need to be cautious about extrapolating from the data. There are some interesting patterns with regard to the high proportion of women on boards, women chief executives, financial turnover and sickness absence rates. There is only one statistically significant finding, which is awkward and will be controversial: that women are more likely to be running the not so high performing NHS organisations.
Find out more
The report will be available from the end of September. For a copy, email andrea.steel@postgrad.mbs.ac.uk.
Also online:
How can the government can promote the value of social enterprises? Ross Griffiths explores how disadvantaged social enterprises are by VAT, where they need more support and why it is possible to adopt a longer-term approach to valuing what a social enterprise brings to the economic, social and environmental wellbeing of an area.



{kind=link}
{kind=link}
No comments yet